This week a very interesting article appeared in the press, including a report by @SarahBoseley in the Guardian. On the face of it, the report she quotes seems to suggest that western countries that had been hit hardest by COVID-19 were those that had the highest levels of obesity and overweight.

When we are faced with a rapidly changing health crisis, it is all too easy to jump to conclusions. This is exactly what some European countries seem to have done in relation to the use of the Astra-Zeneca vaccine. They were forced to make a decision on the basis of incomplete data. Now that the results have come back from UK studies, we have better data and most countries are reconsidering their decisions. But the damage has been done. There are reports of Astra-Zeneca ampules lying unused in fridges across France, people now don’t trust it. Is this a similar case. Is obesity the casue of COVID-19 complication, or just one of the contributory factors?
Since very early on in this pandemic obesity has been linked to poor outcomes from COVID-19. Right at the beginning, in April 2020 a Chinese study looked at 383 consecutively hospitalised patients and found that those with Asian classifications of overweight and obesity (see below) had 84% and 240% respective increased odds of developing severe COVID-19 after allowing for possible confounders.[i] Studies across the world have found similar situations. But the question remains whether obesity and overweight are symptoms of a greater malaise, or whether weight is the golden bullet that explains why some poor countries, particularly in sub-Saharan Africa, have escaped so lightly from the pandemic, where wealthy countries, especially the US and UK, have fared so badly.
This month the World Obesity Federation (WOF) has weighed in[ii]. The cautious will notice that this is a report, not a study or a statistical analysis. It attempts to explains the incredibly sad death rates found in many wealthy western countries by mapping levels of obesity.
What the report shows
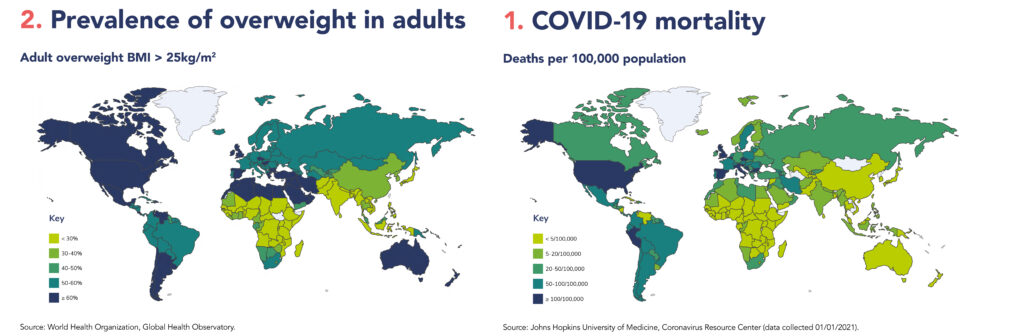
These world maps outline the evidence that has been gathered.
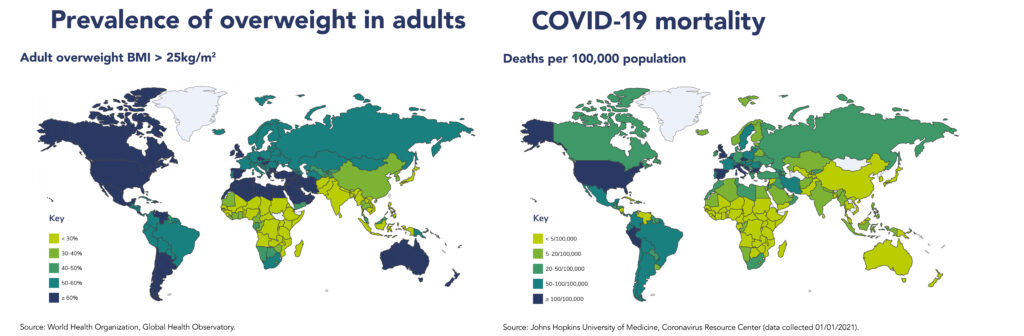
What these maps can’t show
Variations in mortality reporting
A drawback in discussing mortality statistics from COVID-19 is that each country reports their numbers differently. For example, there is some suggestion that Belgium’s statistics are higher because of their scrupulous policy of including everyone with suspected contagion, regardless of whether they had had a test or not. Wealthy western countries have counted fairly copiously – they have an electorate to answer to. But some poorer countries simply don’t have the capacity to test everyone – and thus might miss many sufferers. Totalitarian countries may be more tempted to cook-the-books if figures look frightening.
It is also always worth reading the small print in studies and reports. Death rates represent a moment in time. In this case, the data was taken from John Hopkins University figures on 1st January 2021. That means the rates missed the peak of European and US deaths in January/February this year. Today’s data might show a different picture. Once the vaccine take-up starts to impact, the figures will look different again in a month or so.
Can we trust worldwide obesity figures?
Moving onto scrutinise the obesity figures, it should be noted that very few countries keep accurate overweight and obesity figures, though thanks to the World Health Organisation these categories are universally defined, as >25kg/m2 for overweight and >30kg/m2 for obesity. Instead of applying nationwide statistics, the WHO captures these data by looking at large scale surveys of representative samples of a country’s population. I’m satisfied to see that in the UK the figures look about right. This study assumes that 63.7% of UK adults are overweight and 27.8% obese. But these are only estimates.
Even if we had perfect weight data for the entire world population, the use of a measure such as Body Mass Index is in itself, questionable. Weight is more complicated than that.
Ethnic differences in overweight
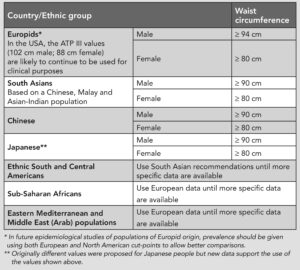
It has been known for a long time that people of different ethnicity have different safe weight thresholds. The Chinese study I quoted at the top of this article used Asian definitions of obesity and overweight, that are different to Caucasian definitions. These definitions are linked to a phalanx of studies that have shown that many diseases and disorders are associated with overweight, such as cardiovascular disease, metabolic syndrome, diabetes and some cancers. The World Health Organisation advises that the definition for people overweight and obesity in Asian populations should be 23kg/m2 and 27.5kg/m2 respectively (WHO 2004), rather than the 25kg/m2 and 30kg/m2 figures that we use for white British people. It is not clear whether variable cut-offs have been chosen for the atlas. Certainly, the listing of the Chinese study does not refer to this anomaly.
Body composition
While Body Mass Index (BMI) is the gold-standard for healthy adults, it becomes a far less useful measure in older people, or in sicker people. That is because weight, per se, has limited use. It is an easy measure, but over time becomes a gradually less useful measure. Issues such as water retention, chronic constipation, osteoporotic stoop and muscle wasting all conspire to render a BMI calculation using weight and height, increasingly irrelevant. A more useful measure would be the amount of lean muscle mass and fat mass. Most studies conclude that it is high fat mass and shrinking muscles mass that together conspire to make us frailer, and more susceptible to infections such as COVID-19.
What is fat mass?
Even the fittest among us have about 25-30% fat. That fat is distributed under the skin, to keep us warm, around the joints, to cushion movement and inside the body, protecting the organs, but sometimes smothering them. Fat found inside the cavity of the torso, called visceral fat, is often measured using waist measurement, but just like BMI, it is subject to gender and ethnic differences. Women naturally carry more fat than men (think boobs and bottoms). Being a dyed-in-the-wool feminist, I prefer in my own clinic to use the rule of thumb that waist circumference should be less than than half height. It is a rough and ready measure, but saves complex discussion of ethnicity and gender stereotyping. A tall woman or a short man would otherwise be penalised. People whose waist measurement is above these safe limits are within the risk-zone for all the disorders associated with obesity, including metabolic syndrome. It may well be metabolic syndrome that is causing these high death rates from COVID-19.
Metabolic syndrome
Metabolic syndrome has a group of symptoms including high levels of blood sugars, poor insulin dispersal and obesity. Visceral fat physically interferes with metabolic function. For example, fat can block insulin secretion by blocking the islets of Langerhans, the cells that secrete insulin from the pancreas. Fat build-up around the intestines can impair elimination, as well as reduce liver and heart function. Visceral fat is associated with diseases such as bowel cancer, diabetes, heart disease, non-alcoholic fatty liver disease and cirrhosis.
How body fat effects disease
Adipose tissue is the body’s main energy store, and was once considered to contain fat cells that simply expanded when we got fat and shrank when we became thinner. But adipose tissue is not just a fuel store. Taken in its entirety, visceral fat, intra-muscular and sub-cutaneous fat work together as an active endocrine (hormonal) organ. Fat tissue is a depository that stores, manufactures and secretes enzymes, hormones and growth factors that in turn effect metabolism, growth and the immune system. Adipocytes, adipose tissue cells, produce and secrete many biologically active substances, sometimes generically referred to as adipocytokines that regulate secretion of cytokines, moderate the immune system, distribute macrophages and lymphocytes that mount the antibody response to pathogens such as bacteria and viruses. [iv] [v] [vi] Overweight and obesity is now viewed as a state of systemic, chronic low-grade inflammation, that interferes with the immunometabolic system.
Electron microscope view of adipose tissue. Live (plump) and dead or empty (shrivelled) adipose cells are held together by a fine fibre of collagen. Living in this maze, between the cells of fat, can be found fibroblasts, white blood cells, nerve endings, and endothelial cells. As fat collects it accumulates a build-up of pro-inflammatory immune cells, macrophages, mast cells, cytotoxic CD81 T-cells and other inflammatory cytokines and neutrophils. The cells are pink due to the presence of a blood supply. This is a working organ, not simply blubber.
When we relate disease risk to obesity, we are really relating disease risk to fat mass. Increasing muscle mass actually helps protect against disease, and builds strength and resilience. Athletes often have a higher-than-average BMI, but lower than average fat mass. They are not at risk.
Why obesity might affect viral infections
We have known for some time that obesity is a risk factor for communicable disease complications as well as non-communicable diseases. We are not used to hearing about risks from communicable diseases, because up to now we’ve been able to use antibiotics and antiretroviral drugs to cure communicable diseases. But with COVID-19, all that changed – almost overnight. The WOF report cites studies that shown that being overweight increases the risk of complications from influenzas, including novel influenzas viruses such as, H1N1 (‘swine flu’) and H3N2. Obesity can also exacerbate other common viral infections, such as blood stream infections, hepatitis, and periodontal infections. Obesity may also reduce the immune response to influenza vaccination[vii] .
How fat is fat?
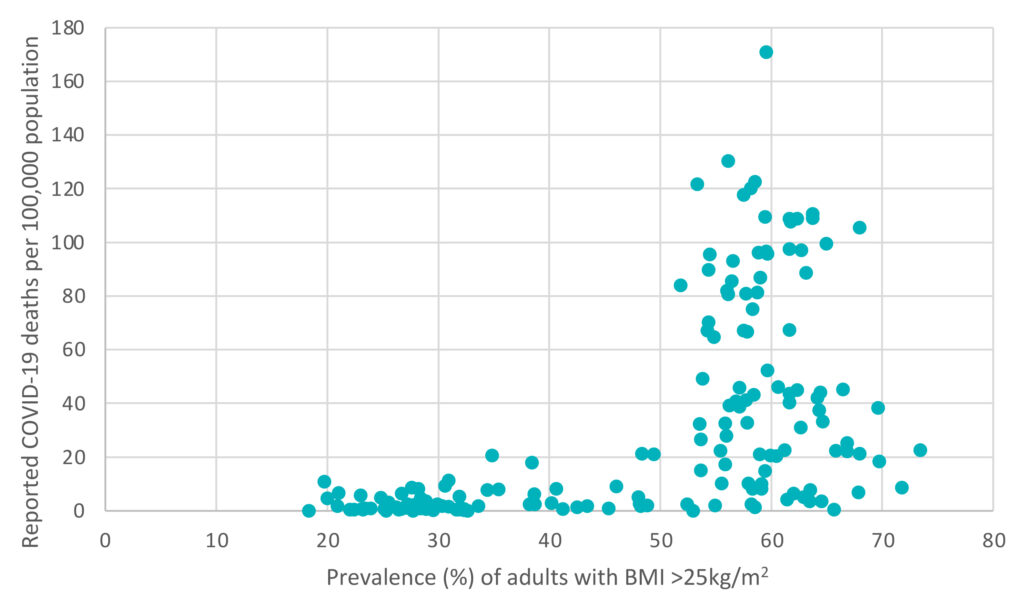
There seems to be a link between the prevalence of overweight and obesity in any given population and the death rate due to COVID-19.
These data suggest that there is a very sudden change in status within countries where more than 50% of the population are overweight. However, while some of these countries show an extremely high death rate, others such as Australia, New Zealand and some Gulf States, all of which possess an unhealthily overweight population, were able to escape high mortality rates.
What else might be causing the difference?
The study examines a series of other contributing factors, for example age, health-care spending, low rates of exercise and high consumption of processed foods. All of these probably have some effect as well. Some studies have equated COVID-19 deaths to vitamin D deficiency, which might explain why poorer, but sunnier countries have fared better than we might have imagined. In addition, stringency of quarantine and lockdown measures, have made a difference. In the future we hope that liberal vaccination programmes, will moderate the death rates even more.
This World Obesity Foundation study is welcome. It is enlightening to see the figures for every country set out with such clarity. But, we need to take the implications, that obesity is the golden bullet, with a pinch of salt. The World Obesity Federation, that published the report, is a lobbying organisation as well as a charity. Its membership is open to anyone with an interest in obesity. That includes many independent scientists, but also includes representatives of pharmaceutical companies with more commercial interests. Top of their mission statement is to see obesity recognised as a disease. This is important for the commercial sector because it means that that obesity treatments can attract NHS funding more easily. And while I have no reason to question the good intentions of the foundation, it should be noted that they are in part funded by and partner with drug companies, such as Johnson and Johnson and commercial diet companies such as Weightwatchers.
In my view losing weight and increasing exercise to ensure low fat mass and growing muscle mass is about the best thing we can do to reduce our long-term risk of complications due to COVID-19, whether we are 25 or 75. Investing in a weighing machine that measures both fat and muscle mass would be a good start. Measuring weight alone, especially after months of enforced lockdown, might offer false security. Many people might have added fat mass (more eating), but lost muscle mass (less activity), resulting in a lower body mass index, but higher obesity risk.
I think weight is important. But we must consider all the other factors that have conspired to make British people so vulnerable to COVID-19. We need to make a whole series of changes, some personal lifestyle changes, but we also need to be changing policies. We need safer working environments, cleaner air, greener space and uncrowded public transport. I doubt very much that one cause will be seen to be the golden bullet. Governments are always looking for simple solutions. But the solution to COVID-19 is about so much more. For me it is part and parcel of changing the way we think about our rights to live a long and healthy life. It is about reducing the iniquities that according to UK figures show a massive increase in death rates due to poverty, overcrowding, public facing work, poor health and safety practices in the workplace and supermarkets. It is easy to see overweight as a personal risk, a choice. But it isn’t. It is part of a complex set of problems that require enduring, wide-ranging, thoughtful and sensitive political solutions.
[i] The regression model for this study included age (per year), sex (female/male), epidemiological characteristics (from Hubei, not been to Hubei, but infected by individuals from Hubei, or without any clear contact history), days from disease onset to hospitalization, hypertension (yes/no), diabetes (yes/no), cardiovascular disease (yes/no), chronic obstructive pulmonary disease (yes/no), liver disease (yes/no) and cancer (yes/no), and drugs used for treatment (lopinavir/ritonavir, favipiravir, and others), as appropriate.
[ii] Lobstein, T, compiler (2021) COVID-19 and Obesity – The 2021 Atlas. Report. World Obesity Federation. March 2021 Available to download from https://www.worldobesity.org/resources/resource-library retrieved March 2021.
[iii] Alberti et al. (2006) The IDF consensus worldwide definition of the metabolic syndrome. International Diabetes Federation, website report https://www.idf.org/e-library/consensus-statements/60-idfconsensus-worldwide-definitionof-the-metabolic-syndrome.html
[iv] Coelho, M., Oliveira, T., & Fernandes, R. (2013). Biochemistry of adipose tissue: an endocrine organ. Archives of medical science : AMS, 9(2), 191–200. https://doi.org/10.5114/aoms.2013.33181
[v] Trzeciak-Ryczek A, et al. (2011) Adipose tissue – component of the immune system. Central European Journal Immunology. 2011;36:95–9
[vi] Itoh M, et al. (2011) Adipose tissue remodelling as homeostatic inflammation. International Journal of Inflammation. 2011;2011:720926. doi: 10.4061/2011/720926. Epub 2011 Jul 7. PMID: 21755030; PMCID: PMC3132651.
[vii] Green & Beck (2017) Obesity Impairs the Adaptive Immune Response to Influenza Virus. Ann American Thoracic Soc. 2017; 14(Supplement_5):S406-S409. doi: 10.1513/AnnalsATS.201706-447AW.
A beta reader is a test reader of an unreleased work (similar to beta testing in software), who gives feedback to the author, from the perspective of an average reader. If you’d like to help me get this book as good as it can be, I’d love to hear from you. You’ve got plenty of time to make up your mind. The chapters will be ready from June onwards. I’m sorry there is no fee for this work, except a free copy of the finished book and an acknowledgement. This is not a commercial exercise. Say Tomato, the publisher of the book and of the website is run as a self-financed social enterprise. I shall be eternally grateful. Any profits from Glorious Summer will be directed into Say Tomato’s work for women over 40.
Contact me directly wendy@wendyshillam.co.uk if you are interested, giving a brief description of yourself and your reading experience. (It doesn’t matter if you haven’t done any beta reading before – avid readers make the best beta readers.) Thank you.

Wendy Shillam
Trained in environmental and bio-sciences, Wendy Shillam is a registered clinical nutritionist, specialising in longevity. She is the founder of the social enterprise Say Tomato! that provides free and trusted weight loss advice for women over forty. This part of the blog is a precursor to publication of her book, Glorious Summer – the secrets of longevity. You can read about it here.
Fascinating as ever. Never thought of fat as anything other than largely bad stuff that just accretes in the body as it does in sewers but amazed to learn it is far more important role than mere insulation / energy store. It seems the media ever seek in our behalf to constrain experts to giving a binary response to any situation, e.g. it is safe or it is not safe; it is right or it is wrong; it is black or it is white. But as you say, no golden bullet answer here either, rather, a complex picture and solution to unravel.